 Montse Moharra. OIGS AQuAS
Montse Moharra. OIGS AQuAS
The Catalan health system is the result of a remarkable historical reality that favours the consolidation of a system characterized by public funding, multiple provision and integration of all resources in a network of public use, which makes it a reference and innovation source in management.
In this context, in 2012 the Observatori d’Innovació en Gestió de la Sanitat in Catalonia (OIGS) (The Centre for Innovation in Health Management in Catalonia) was created with the aim of collecting and giving value to the knowledge generated by innovative initiatives: innovative experiences, strategic partnerships and best practices. Currently, OIGS includes a total of 181 experiences, of which 56% are related to the management of healthcare and strategic processes, 14% with chronic patients, 14% with TIC and 7% drug related.
OIGS also offers an innovation learning space through a public portal and a community of innovation that facilitates the interaction between over 400 professional users who are already sharing their experiences.
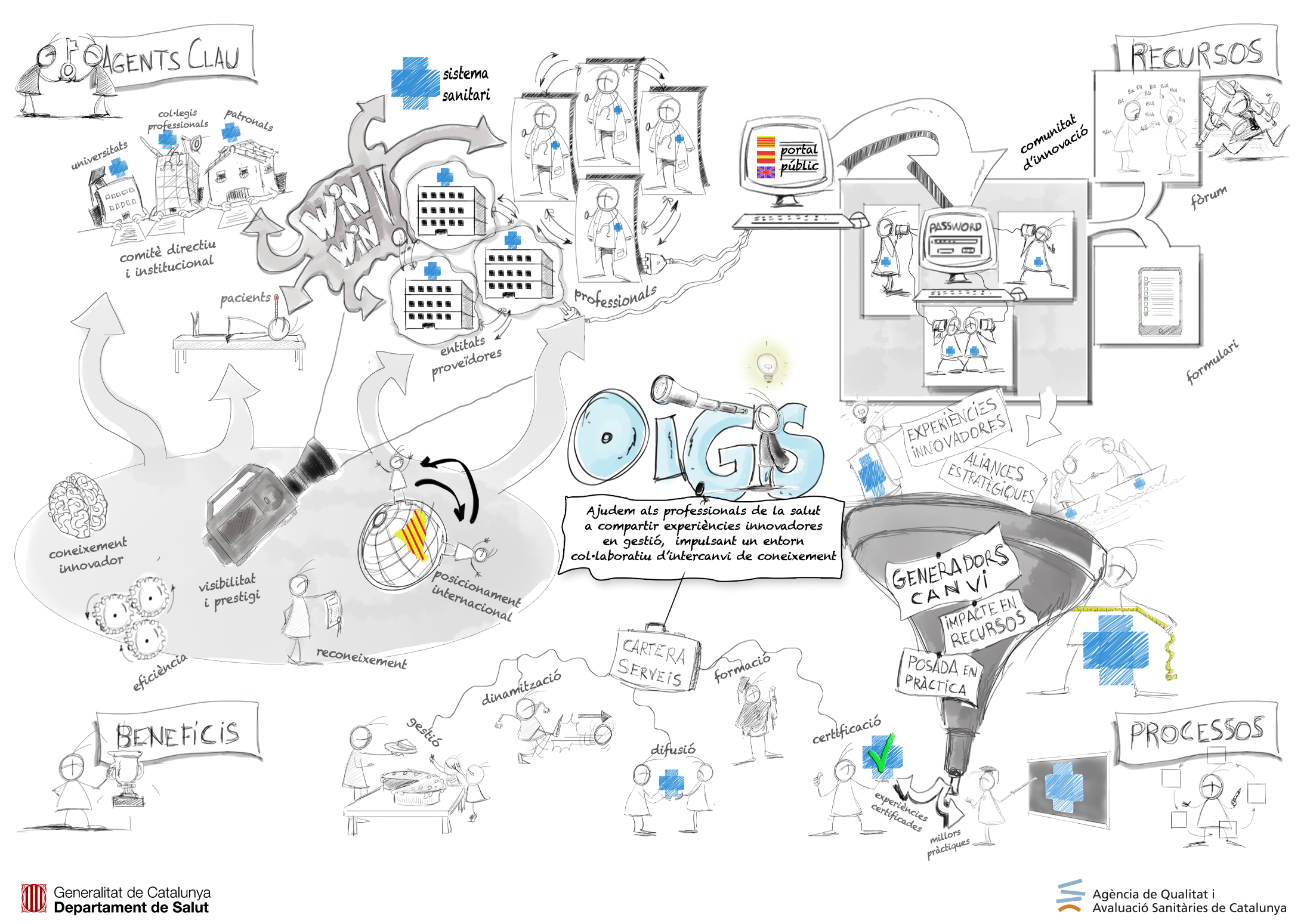
How can an innovative experience be registered?
One has to register with the innovation community and fill in a form with the experience data. The form content is reviewed by the OIGS and the experience is published on the website if it meets the established criteria: having been implemented within an organization, generating a change, having had an impact on resource optimization and being expansible to other organizations or systems.
When the experience is published, the willing organizations may present at any time, also through the innovation community, the self-assessment of the experience. OIGS reviews and evaluates the presented self-assessment and those experiences that exceed this evaluation, obtain a quality certificate issued by AQuAS. Thus, so far 19 experiences have been certified.
Identifying the best practices in health management
Starting from the process of reviewing management innovative experiments, identifying commonalities and required by CatSalut, so far three potentially scalable experiences throughout the healthcare system have been identified: the suitability of prescribing in primary and community care; the online preoperative and the online dermatology. However, this is an ongoing process that ought to facilitate identifying new best practices.
OIGS in the future
In the near future, OIGS aims to encourage the participation of professionals and organizations that are important to system innovation; to create knowledge networks through participation in research and innovation projects at European level and organizing specific thematic workshops. The innovation community will facilitate identifying experiences that can be part of potential interest groups and that will be able to respond to the specific challenges related to European funding such as innovative public procurement.

 Jordi Varela, Editor of the blog “Advances in Clinical Management“
Jordi Varela, Editor of the blog “Advances in Clinical Management“ Paula Adam,
Paula Adam, 


 Anna García-Altés
Anna García-Altés





