Research impact assessment studies show that to achieve more impact on society the participation of ‘people that can provide value’ is an important factor. What these studies show us is that making key actors participate in the long process of research can improve the efficacy of its application and its impact on society. In the conference which AQuAS organised on Participation in Research last April 4, Derek Stewart, very much involved in Patient and Public Involvement and Engagement at the NIHR Nottingham Biomedical Research Centre, told us that participation provides different perspectives to research. In addition, Derek Stewart explained that “while patients have the opportunity to configure the future and make sense of what is happening to them in their day to day, researchers have the opportunity to legitimate what they do and make their results visible.”
So what have we learnt from all this? Firstly, that there is diversity of participation in research with a wide range of ways of interaction that are inserted in the different levels of the research process. Secondly, that despite individual idiosyncrasies, a global and shared approach is needed to avoid contradictions and to take advantage of mutual learning. Thirdly, that a commitment is needed on the part of all the different institutions and the research community in order to favour participation in research and to have an impact on society. This is why a Work Group on Participation in Research has been created, (#SomRecerca). Under the initial coordination of AQuAS, different health research institutions have come together to promote actions, agents or strategies that facilitate participation and that foster more awareness of the research community. The principles that accompany this group are based on mutual support and the acceptance that diversity and different realities exist within each context.
The first step taken by this group has been to hold conferences in two institutions (IMIM and IDIBELL), last 22 and 23 of January, under the title Shall we go one step further? Placing the patient at the centre of research. These conferences have been a good opportunity to present experiences that were already on the go within the institution itself which place the patient at the centre of research.
The conferences have made the different experiences stemming from individual motivations worthwhile, of researchers or users themselves, and they have been inspirational as examples of where one can start. The patient has been placed at the centre of research in these experiences: to obtain resources, to generate ideas, to prioritise research or to be a part of the research team, among others.
And more specifically, actions have been proposed that help develop the participation of patients which provides value in research:
Informing patients of the research that is being carried out in institutions; that is, bringing research closer to citizens
Communicative skills of the researcher towards a non-scientific audience
Effective communication channels between patients and researchers, be they via an associative network or via other activities or means of communication such as conferences with patients, etc…
Support for all those involved in participation: of recruitment, of time, of resources, between researchers or with a guide.
Stable work groups that include the participation of different profiles (basic and clinical researchers, assistants, managers and patients) so as to identify needs, come up with ideas or make proposals, for example.
In short, the synergies between patients and researchers must be sought out in those cases where value can be provided. It is not always and easy path but one which makes a whole lot of sense.
The need to place the patient at the centre of the model of care is widely accepted and is thus reflected in the Health Plan. Meeting this need is a substantial improvement in services and involves changes in the way these services are provided and that is precisely what innovation is all about.
What is needed, therefore, is to ask ourselves what instruments we have to incorporate innovation in public services and facilitate this change of model.
The RITMOCORE project, coordinated by the AQuAS, is in fact a public procurement of innovation initiative which aims to incorporate innovation in the provision of services to patients which carry or need a pacemaker. The end aim is to achieve care of higher quality, more personalised and ultimately, of more value for those patients who have been fitted with a pacemaker.
Public procurement has revealed itself to be a lever for change regarding the model of provision and organisation of health services and of the relationship with providers. This is why the AQuAS has driven several initiatives at a Catalan and European level in this area, such as numerous European projects or the recent call by CatSalut for PPI projects.
Catalan hospitals (Hospital Universitari de Bellvitge, Mútua Terrassa and the Hospital Sant Pau) and English hospitals (Liverpool Heart and Chest Hospital and Countess of Chester Hospital) have undertaken a joint bid under the clinical and administrative leadership of Hospital Sant Pau, and coordinated by AQuAS which will be published at the end of 2018. This bid will make it possible to contract a service that will make the tracking of all patients with pacemakers effective and stimulate their activation, and it will enable the selection of the most appropriate devices for each patient, promote the coordination between levels of healthcare and permit the management of change of the ICTs that are needed: an integral service in line with what the health plan requires.
This inspiring project provides a practical approach to everything regarding the key issues in re-orienting the model of care. It forces us to deal with the constraints of the regulatory framework of public procurement and make continual assessments of risk, but above all, RITMOCORE forces us to manage the complexity of multidisciplinary environments (medicine, nursing, contracting, finances, etc…) that provide a very enriching opportunity and a challenge at the same time.
Complexity is inevitably a source of innovation. Providing ourselves with the instruments to exploit all the potential in favour of the care of people is our responsibility. Society, the healthcare environment and collaboration with the private sector are highly complex realities which offer the opportunity to generate, adopt and spread innovation.
La necesidad de poner al paciente en el centro del modelo de atención está ampliamente reconocida y así se recoge en el Pla de Salut. Dar respuesta a esta necesidad es una mejora sustancial de los servicios e implica cambios en la forma que se prestan estos servicios y ésto esprecisamente la innovación.
Así pues, lo que hay que hacer es preguntarnos qué instrumentos tenemos para incorporar la innovación en los servicios públicos y facilitar este cambio de modelo.
El proyecto RITMOCORE, coordinado por AQuAS, la Agencia de Calidad y Evaluación Sanitarias de Cataluña, es justamente una iniciativa que pretende incorporar innovación en la provisión de servicios a los pacientes que llevan o necesitan un marcapasos a través de la compra pública de innovación, a fin de lograr una atención de más calidad, más personalizada y en definitiva más valiosa para aquellos pacientes que llevan un marcapasos implantado.
La compra pública se ha revelado como una palanca de cambio para el modelo de provisión y organización de servicios de salud y de la relación con los proveedores, es por este motivo que AQuAS ha impulsado varias iniciativas a nivel catalán y europeo en este ámbito, como numerosos proyectos europeos o la reciente convocatoria del CatSalut para proyectos de CPI.
Hospitales catalanes (Hospital Universitari de Bellvitge, Mútua Terrassa y Hospital Sant Pau) y hospitales ingleses (Liverpool Heart and Chest Hospital i Countess of Chester Hospital) emprenden bajo el liderazgo clínico y administrativo de Sant Pau, y bajo la coordinación de AQuAS, una licitación conjunta que se publicará a finales de este 2018. Esta licitación permitirá contratar un servicio que haga efectivo el seguimiento remoto en todos los pacientes con marcapasos, que fomente su activación, que permita seleccionar aquellos dispositivos más adecuados en cada paciente, que facilite la coordinación entre niveles asistenciales y permita la gestión del cambio con las TIC que sean necesarias: todo un servicio integral en la línea de lo que reclama el Pla de Salut.
Este estimulante proyecto permite tratar de forma práctica cuestiones cruciales para la reorientación del modelo de atención y obliga a afrontar los condicionantes del marco regulador de la contratación pública, hacer contínuos ejercicios de evaluación de riesgos, pero sobre todo, el proyecto RITMOCORE obliga a gestionar la complexidad de entornos multidisciplinares (medicina, enfermería, contratación, finanzas, etc.) que representa una oportunidad muy enriquecedora y un reto a la vez.
La complejidad és indefectiblemente una fuente de innovación y dotarnos de instrumentos para explorar todo su potencial en beneficio de los servicios a las personas es nuestra responsabilidad. La sociedad, el entorno asistencial y la colaboración con el mundo privado son realidades altamente complejas y nos ofrecen contínuas oportunidades para generar, adoptar y extender la innovación.
For years, I have been under the impression of not having a clear idea of how information related to the complex world of medicine and health should be disseminated in the daily news media, both of the science that it is based on and of the difficulties and dilemmas in applying it in practice.
I have repeatedly refused offers, with only rare exceptions, to write texts on these subjects in newspapers or books of a non-professional nature: I had serious doubts of how to transmit this knowledge to the public at large. Looking back critically on these reservations I have had, I think they have been related to the paternalism inherent in the medical training received by the professionals of my generation: the fear that the public will make an incorrect interpretation and come to abhorrent conclusions of the facts disseminated, an audience with little knowledge on the theoretical foundations and subtleties of these facts, which are only accessible with proper professional training. Indeed, experience has shown me that these reservations were indeed justified.
However, at the same time, I have witnessed the growth of citizens’ autonomy, now widely acknowledged, and their right to take “informed decisions”. This position, which has come to define the 21st Century as “the patients’ century”, acknowledges their right to know relevant professional data so as to be able to take accurate decisions autonomously; it has an undeniable foundation but if we are to avoid that this leads to the proliferation of distorted facts it will require a rigorous preparation and an absence of spurious interests on the part of those divulging information. Ideally, these informants should contribute to “health literacy” in a way that is balanced, objective and unemotional.
The tension between these two conceptions of health information goes in parallel with that which exists between two extreme views of the doctor-patient relationship: the classical paternalistic one (“the doctor knows better than anyone what is best for a patient and their decision must be accepted”) and that of the “informed consumer” with autonomous decisions. The other extreme of this corresponds to an “imminent revolution” in which it would be the very well-informed patient, (basically as a result of the spread of refined computer technology) that would take the most important decisions concerning themselves.
Personally, like many others, I prefer a more balanced approach: that corresponding to the “interpretative” and “deliberative” models of the doctor-patient relationship, in which the experience and knowledge of the former interact with the latter respecting their autonomy.
I think that this dilemma runs parallel to the medical information found in daily news media: on the one hand, there is the social demand to inform citizens of current advances so they know their options or opportunities as “informed consumers”; on the other, there is the temptation to fuel the emotions (triumphalism or fear) of the reader who is untrained by offering them information which is largely uncritical, lacks rigour or is insufficient, with the risk of a biased, distorted or exaggerated interpretation. The more or less unreal notions that some informants may have on medical and health problems (common, alas, among many professionals) can be transmitted like this directly to the citizen and to their emotions and desires.
In the case of news related to medical advances and innovations, I would like citizens to know what expectations these novelties raise, maybe now within their reach, and the magnitude or relevance of the problem that can be lessened or resolved, and that this be done by using a rigorous and prudent terminology so that citizens can also create their own opinion on the solidity or temporariness of an innovation, and of the related uncertainties and limitations: not only of the benefits that they can provide them with but also of the undesired, uncomfortable or harmful side effects they might produce, and whether they are in anyway frequent or probable. In other words, I would not like the main aim of this information to be that of creating hope or fear in the reader, or give them the idea in a triumphal tone that in the wonderful world of science, the war against disease has claimed a new victory, especially at the hands of local researchers.
Even though some well-documented news described in sufficient detail was found that could provide balanced information to the reader in this analysis, in many other cases the information was one-sided or not very thorough and was devoid of facts related to questionable aspects of the innovation and their risks. It resulted in a biased message which often tended to induce optimism in the reader rather than educate them in the knowledge of the pros and cons of the medical innovations.
At a time when there is a call for a user’s well-informed autonomy, I would be delighted if healthcare culture and the attitude of the news media did not amount to a paternalistic doctor-patient relationship. In this regard, there is no doubt that much still needs to be done.
Post written by Gaietà Permanyer Miralda. Emeritus physician. Unit of Epidemiology, Cardiology Service. Hospital Vall d’Hebron, Barcelona.
The aim of the Essencial Project is to improve the quality of healthcare by providing professionals with evidence that is useful for them to make informed decisions in their day to day work.
What is special about this project is that this is done by identifying routine low-value practices in the health system and by using a strategy aimed at avoiding these practices.
Cari Almazán, the person in charge of this project, responds to questions in an interview.
What is the Essencial Project?
It is a project of the Department of Health of Catalonia led by the Agency for Health Quality and Assessment of Catalonia (AQuAS – its Catalan acronym), in which researchers from the AQuAS, health professionals, scientific societies and the Advisory Board of Patients participate. Each and every one, in their role, work with a clear objective: improving the quality of healthcare using a very specific strategy to identify low-value practices and thereby provide information to professionals to help them avoid doing all the things they do which do not offer any health benefits to the patient.
What is a low-value practice?
In usual medical practice, there are known routines that do not offer any benefit to the patient and it is difficult to understand why these occur but it is even more difficult to try and avoid them. In all likelihood there is a resistance to change and we need to spend a lot of time explaining what this project is about.
How does the Essencial Project work?
It works at different levels and we try to be systematic and transparent. This involves a line of work which includes: identifying low-value practices, finding knowledge (the evidence), informing about and implementing the project.
If a routine does not offer any benefit to the patient, why is it followed?
This is precisely what we ask professionals in primary care, among many other things. The comments “because we have always done it like this” or “because it is a request of the patient” are frequent. There is a certain tendency to want to feel we are being useful, a human one I would say. Both the professional and the patient feel better but on occasion, there is evidence which indicates that this “feeling better” is not accompanied by any benefit for the patient. This is what needs to be explained very carefully.
What role does the Essencial Project have in the day to day activity of a health professional and that of a potential patient?
There are many projects aligned with the initiative to improve the quality of healthcare. In this context, the Essencial Project is a tool of the health system to help health professionals make decisions. The Essencial Project thus aims to be useful to the health system and professionals. In addition, for a potential patient, knowing about this project can also help contribute to their understanding of why a health professional does not recommend a certain diagnostic test or treatment.
I am unsure as to whether the project is aimed at professionals or at citizens.
The Essencial Project is aimed at the entire population. On the one hand, it is aimed at professionals to provide them with this tool, but also at citizens. Why not? Whether citizens want this information is another thing altogether.
Do citizens show an interest in having all this information available to them?
We don’t know, we should ask them. We know of experiences where it is not clear that the information which is given is the information that citizens want but at the AQuAS we believe that sharing knowledge and methodology is an exercise in responsibility.
Who chooses the recommendations?
Cari: They are chosen in collaboration with the different scientific societies. Right now, there is a participative process on the go to prioritise low-value clinical practices in the framework of the Third Conference of Care in Sexual and Reproductive Health. In the Essencial Conference 2017 subjects for recommendation were prioritised based on the participation of the professionals that attended the conference. The idea is that it is the professionals themselves who identify when and where practices of this sort occur.
Who creates the contents of the Essencial Project?
The contents that accompany each recommendation are the result of the participation of many expert professionals in different disciplines. These contents are then validated. In terms of the videos, professionals at the AQuAS along with health professionals produce these which explain the key idea of each recommendation in the first person in an informative manner.
What would you highlight of the Essencial Project?
That we offer every recommendation, the chance to collaborate with health professionals, a bibliography and files for patients in a systematic way. This last idea of files for patients is a subject which we will delve into more deeply shortly from the agency. Perhaps, what I would say is most important here is that all this forms a part of a commitment to bring the culture of assessment and the culture of Choosing Wisely at all levels closer to everyone: the citizenry, professionals and the health system.
Developing a platform based on mHealth that has mobile applications (apps), a game and intelligent sensors has been the goal of the European project PEGASO Fit For Future, which began in December 2013 and ended last July.
It is a platform that aims to improve both the lifestyles of adolescents (diet, physical activity and hours of sleep) and the knowledge that they might have about these life styles. To achieve this, intelligent sensors (t-shirt and bracelet) which record the physical activity and hours of sleep of an individual and also different apps which record the intake of food by means of a diary and footsteps taken by means of an accelerometer were developed and tested.
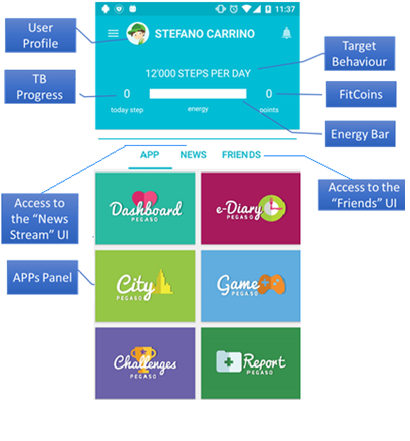
The PEGASO Fit For Future platform detects which lifestyles a user has and makes recommendations on how to improve them. In addition, it incorporates a gamification component: based on how healthy the lifestyle of a user is as well as how much their knowledge improves, which are then converted into obtaining a greater or lesser amount of points.
As an example, here we can see a screenshot of a fictitious user:
Professionals from different areas collaborated in the project: developers of games, apps and sensors, design and gaming experts, health professionals (doctors, nurses, experts in nutrition, experts in physical activity and psychologists) and also experts in health technology assessment and public health.
There were two different phases of the project: the development phase of the platform and the assessment phase.
During the development phase, while some professionals put their efforts into ensuring the quality and appropriateness of the medical and clinical content of the platform, others concentrated on aspects of a technological nature.
Nevertheless, the opinions of the end users themselves, adolescents, were always kept in mind during this process. In three iterative stages, boys and girls in Catalonia, Lombardy, England and Scotland tested this technology out in the different stages of its development.
The proposals for improvement made by the adolescents including their preferences were, whenever possible, kept in mind for the later versions of the platform. The aim was to guarantee as far as possible that what was being developed was practical for and accepted by the end users.
The last stage of the project was the assessment of the platform. The assessment of the different elements (apps, games and sensors) was to see if they really did help to improve the lifestyles and knowledge about lifestyles among adolescents and to assess the experience of the user after having used the platform.
To this end, a pilot study was carried out with adolescents from Catalonia, Lombardy, Scotland and England in which 365 mobile phones with the PEGASO platform installed were used by adolescents.
After six months of use, the intervention was assessed by means of validated questionnaires, a qualitative methodology and data obtained from the platform itself. A control group was introduced allowing for comparisons to be made with adolescents that did not have access to the platform.
The results of this study will help to evaluate whether new technologies are practical in helping adolescents improve both their lifestyles and knowledge about these lifestyles, a population group accustomed to using new technologies and that, in general, do not often visit health professionals.
Getting closer to the population by using mobile technology and the recreational aspect of gaming could be a good strategy for an intervention of this type related to the promotion of healthy lifestyles among adolescents. At a population level, it is a long-term strategy and hence the slogan “Fit For Future” of the PEGASO project.
Assumpció González Mestre, Head of Programa Pacient Expert Catalunya® (Expert Patient Programme Catalonia®) and Cuidador Expert Catalunya® (Expert Caregiver Catalonia®) answers questions in an interview with Cari Almazán related to the figure of “expert caregiver”.
The programmes of Pacient Expert Catalunya® and Cuidador Expert Catalunya®, respectively, have the same aim of equipping people with the tools and resources to help them in their daily lives.
This type of learning programme among equals manages to improve the quality of life of people which find themselves in the environment of a disease in the context of chronicity in Catalonia, be it as patients, as caregivers or both things together.
Cari: Who is the Programa Cuidador Expert Catalunya® aimed at?
Assumpció: Our field of action is clearly orientated at the caregivers of people having chronic diseases. By “expert caregiver” we understand them to be a person who takes care of another person with a chronic disease having complex attention needs and who is able to take on that responsibility, give care and acquire the skills that help them manage the physical, emotional and social impact of giving care thereby improving their life quality and that of the person they are taking care of.
Cari: What does turning a caregiver into an expert caregiver involve?
Assumpció: When a person finds themselves in the situation of having to take on the task of taking care of another person with a disease, the life of that person is totally conditioned by the situations, planned or not, foreseen or unforeseen, which the disease might involve. Helping a person in that critical moment often generates a change in the life of the person giving care and it becomes an emotional overload in their daily lives as a result of having to address the needs of the person they are taking care of. In this sense, having more capacity to take on responsibility and being able to take care of themselves and of the other person, on the one hand, and of acquiring skills that help them manage the physical, emotional and social impact which we know this situation involves, on the other, are some of the key aspects that we would consider as essential when identifying a possible expert caregiver.
Cari: Is being able to improve the quality of life of caregivers the aim of the programme?
Assumpció: It is one of the main aims although there are others. Giving support to caregivers in the management and care of the person they are taking care of; improving the life of caregivers; being able to involve and satisfy patients and caregivers; improving the efficacy of caregivers in their own care and in the care of the person they are taking care of; learning to identify the degree of overload on caregivers; and having an influence on aspects of the health of a caregiver related to giving care, are the six specific aims of the Programa Cuidador Expert Catalunya®.
Cari: Should all caregivers become expert caregivers?
Assumpció: The end goal is not that everyone becomes an expert but rather that they become aware of what it means to be a caregiver and to learn to identify when they find themselves overloaded and that, therefore, they need to ask for help from another person of the family or from a professional to be able to deal with the situation which they find themselves in. If caregivers become aware of this situation and ask for support at the appropriate time, they will be able to give care and take care of themselves better. Therefore, the expert caregiver is a volunteer with the capacity to take care of themselves without psychophysical disabilities and who can empathise, be interested in helping, be highly motivated and have strong communicative skills. These elements are assessed in an individual interview and after completing specific questionnaires.
Cari: Perhaps it is not always easy to put oneself in someone else’s shoes…
Assumpció: One of the fundamental aspects of this initiative and one which makes it different is that the expert caregiver experiences caregiving first hand which places them in a privileged position when talking to other people who are going through similar experiences.
Cari: What role does the health professional play in relation to the expert caregiver?
Assumpció: The health professional (doctor, nurse or social worker) takes on the role of observer, who can step in to redirect the session, but only when necessary. The Cuidador Expert Catalunya® programme helps both people to closely collaborate with each other having the same aim: to improve the quality of life of the patient, the caregiver and their environment.
Cari: What are the basics of the programme in terms of content and who developed them?
Assumpció: The specific educational materials and methodological guide are the result of the participation of a lot of expert health professionals from different disciplines. These contents have later been validated with the participation of caregivers. The idea is to get to people and so an appropriate language for everyone is needed.
Cari: How has theCuidador Expert Catalunya® programme been implemented?
Assumpció: The process of implementation in a care team involves different stages which include the presentation of the programme to professionals, the selection of caregivers, the training of professionals and caregivers, the setting up of the group of caregivers and the start of sessions.
Cari: In summary therefore… what it is about, in the end, is to organise sessions?
Assumpció: Not exactly. It is about sharing knowledge and experiences among caregivers through 9 structured sessions where they approach and deal with a different subject each day looking for the tools that aid them to take care of themselves.
Cari: How is theCuidador Expert Catalunya® programme assessed?
Assumpció: It is assessed quantitatively and qualitatively by measuring the knowledge gained, the degree of self-care, quality of life, self-reported problems, the degree of overload, the degree of satisfaction and the use of services. The results between the start and end of the intervention are compared and then again 6 and 12 months after it has ended.
Cari: What is the key element of the project?
Assumpció: Without a shadow of a doubt, learning among equals and the relational network. Throughout the experience acquired during the implementation of the programme, we have had the opportunity to confirm that the fact that the programme takes place in one neighbourhood or community is very positive. The relational network between the people that participate in the different groups makes it possible for the expert caregiver to become an agent in the community. The programme becomes a community activity of learning among equals.
During the fifth edition of the international Preventing Overdiagnosis Congress, strategies for implementing solutions to avoid overdiagnosis and overuse were addressed based on the available scientific evidence.
In this year’s edition, which was held in Barcelona last year, apart from the involvement of professionals and organisations, patients had the opportunity to actively participate.
Experiences in different healthcare areas were shown in the use of best practices to communicate and to empower patients to achieve a better understanding of shared decisions.
Different world initiatives addressed the best practices to empower citizens in subjects related to low value practices, overdiagnosis and overtreatment. Experiences were shared and a debate was initiated on fundamental subjects such as the communication and participation of patients.
In recent years, the Essencial Project has studied the perspective of health professionals on low value practices, their causes and possible solutions so as to avoid them.
Essencial Project team: Cari Almazán, Johanna Caro, Liliana Arroyo and Hortènsia Aguado
For example, in a previous post, we explained the results of a survey we carried out with professionals in the field of primary care. The results of this survey highlighted the need to involve and empower the population more. Patients are also important decision makers in relation to their needs and in the demand for certain health services. Hence, the project must be accompanied by a communications strategy aimed not only at patients but also at citizens in general.
That is why we, from the Essencial Project, have been interested in finding out the opinion of patients in addition to the perspective of professionals. In the international Preventing Overdiagnosis 2017 Congress we participated explaining how an exploratory first approach was made to identify the beliefs, attitudes and perceptions of patients regarding the most important elements in consultations, low value practices and the essential components of an effective dialogue between professionals and patients. The end purpose of this was to understand the position of people before initiating possible interventions in the citizenry and to determine the most effective communicative tools and channels.
In Catalonia, AQuAS carried out the first exploratory qualitative study at the end of 2016 using a focus group of parents and children assigned to a primary care team. Low value practices in paediatrics are frequently associated with an over-diagnosis regarding antibiotics, bronchodilatadors, antipyretics or imaging tests, among others. These scenarios have been transferred to the debate with patients themselves. In total, seven women, mothers and grandmother of 14 children participated.
The first point of discussion was the most important elements in a consultation with health professionals and it was found that the treatment (29%) and information received (28%) are the most important elements received by professionals (representing approximately 60% of those mentioned). The relationship with the professional comes next (15%, often related to the degree of trust), followed by the feeling that their wishes or needs are met (12%), information requested (9%) and the diagnosis (5%).
The participants did not know the concept of low value practice but did recognise situations of an excessive prescription of medication or the request of unnecessary tests, especially in emergency services and private consultations.
Regarding communication, the participants said they appreciated that professionals communicate in a simple and direct manner, explaining the reasons for decisions. Similarly, that they felt it was important to receive printed information from professionals which they could peruse later at home. They also said they would like more informative sessions or community groups where these types of subjects could be explained to them and so gain more knowledge about these types of practices.
In our context, this is the first exploratory study done to identify low value practices and the communicative strategies of the citizenry, being the start of a series of studies on the population. Nonetheless, one of the limitations with which we find ourselves was that the participation was lower than expected. Although the term ‘low value practices’ is not known, participants identify situations in which they have experienced them.
Similarly, it is important to underline how patients value the treatment and information received as well as the professional-patient relationship. In the same way, patients recognise the need for a professional’s communication skills and the need for tools to support an effective communicative exchange.
Post written by Johanna Caro Mendivelso (@jmcaro103).
It is very common to see groups of people looking at their mobile devices in any place at any time: on holiday, at work, at home, in the underground, on the bus, in a congress, ….. wherever. It is also common to take advantage of our holidays to say that we will make the most of these days to disconnect from our routines. Does this include disconnecting our mobile phones, tablets, laptops, the TV or email?
At AQuAS, as an agency involved in health assessment, we do not know this. What we do know is that there is more and more talk of connected health, a term which includes mHealth, eHealth and all related concepts, which have been a part of everyday life for some time now.
At a level of the Catalan system of health, we have in this post by Òscar Solans an example of the development of technological tools which involve new ways of interaction between patients and the health system. In this way, La Meva Salut and eConsult are useful tools when placing the patient, the person that is, at the centre of all the interactions there are with the health professionals coming from different fields.
At a European level, Jean Patrick Mathieu and Rossana Alessandrello wrote about how complex the subjects of interoperability and the implementation of mobile technological solutions are, in this other post. This was the framework for the European project DECIPHER whose goal was to facilitate the access to health information from different countries and health systems.
Let’s change the perspective. At an individual level, who does not have an app downloaded on their mobile phone? Which of these apps have to do with something related to health, such as weight control, for example, or as support when doing physical exercise, to keep track of menstrual cycles, fertility calendars or aspects of mental and emotional health? And no need to limit ourselves to talking about mobile devices: who has not heard of calculators for aspects of health such as calculators of life expectancy?
Downloading an app is very easy and can even be free. In this post by Elisa Puigdomènech, she highlighted the fact that in mid-2016 The Economist explained there were some 165,000 apps related to health. This figure must no doubt have increased.
What does the success of an app depend on? What guarantees of quality and safety do they offer?
Regarding the first question, the user experience was the subject on which Elisa Puigdomènech put the emphasis, based on the experience obtained in the PEGASO project. Along the same lines, Santi Gómez spoke about the fact that the development of a health application must, in all phases of its development, include the participation of those who will ultimately be the end users.
And in terms of the second question, any health intervention should be safe, be based on evidence, on the best quality knowledge available and should be assessable. This is the premise with which we at the AQuAS work and this is the role that an assessment agency can play when thinking about connected health. Thus, this post by Toni Dedéu places the emphasis on the fact that technologists, assessors, professionals and citizens have the opportunity to work together and combine their expertise but not forgetting the speed of innovation.
In conclusion, the assessment of connected health is a current topic. This article was recently published, and is a good example of a proposal for a conceptual framework. We end this post with an editorial about innovation and evidence which invites one to reflect on assessment and innovation.
I was recently in Barcelona talking to a group of people interested in the taking of shared decisions (#decisionescompartidas) at a seminar organised by the Catalan Society for Health Management (SCGS) and the Agency for Health Quality and Assessment of Catalonia (AQuAS). My visit was the third stop on a trip which first took me to Poland and later The Netherlands. There is a very strong interest in the subject of shared decisions in all three countries and in all three there are efforts at different levels to promote this practice.
What motivates this interest is also something shared: the feeling that the involvement of patients in important decisions must inevitably reduce costs and improve clinical outcomes. It is also a general phenomenon that doctors feel cornered by this new expectation adding to their already existing agendas that compete for the meagre 7 minutes per patient.
In light of this reality, the promises to take shared decisions that better reflect the situation of a patient and how to deal with it, based on the informed participation of the patient, end up putting the onus on the patient of taking decisions by means of tools in web pages or on printed forms. But what about sharing the process of taking decisions? Corporate poetry, an academic dream.
Taking shared decisions requires patients and clinicians to work together so as to mutually agree on the best way to proceed in order to improve the patient’s situation. The outcome of this effort is a plan of care. To establish this plan it is important to understand what the situation of the patient is and what action is needed, as well as the options available to respond to the demands that the situation dictates in the best way.
The conclusion reached must make sense, intellectually, emotionally and practically. That is, the plan must reflect the best medical science, it has to be agreeable within the biological and biographical circumstances of the patient and be able to be implemented with the least possible inconvenience in the life of the patient. This work is not for the patient to do, nor the clinician, but for both. It is challenging and is based on a clinician-patient relationship, and it takes time.
Many clinicians tell me that they already take decisions together with their patients. This is not evident when we watch videos of clinical encounters in North America (15-30 minutes in length). In these, we see clinicians interrupting patients after less than 11 seconds from the time a patient begins talking, using humour to avoid emotional situations and offering recommendations before listening to the patient’s point of view.
Victor M.Montori in the Shared Decisions Conference (SCGS and AQuAS). Barcelona, 19 May 2017
The fact that patients want to participate or that they do in fact participate actively in the taking of decisions is not evident either and yet, patients report high levels of satisfaction in the way that decisions are taken. However, a critical look reveals that many decisions are taken without patients realising it, given that these decisions are disguised as the logical steps to follow in managing a problem rather than being opportunities for the patient to contribute in the process with their opinion, point of view, experience and knowledge.
The effort of converting the taking of shared decisions from what it is (a unicorn) to what it should be (something routine in the care of patients) is enormous and full of uncertainty. There is no country, in my opinion, nor any health system which is at the forefront on this subject. At the tail end, there are of course countless systems that are still hugely in debt with their populations for not yet having been able to guarantee universal access to health with minimum levels of quality and safety.
What those at the forefront need to do, in my opinion, has more to do with attitude and opportunity than with tools or incentive and training programmes. The latter must be there when attitude and opportunity appear.
In my visit to Barcelona I saw great willingness, but with noticeable limitations in attitude and opportunity. In attitude, as health professionals we need to value what patients know about their context, about their biology and biography and about the way in which they want to lead their lives.
We must acknowledge how essential it is that treatment plans make sense and that it is possible to implement them in the lives of patients, especially in the case of chronic patients. And we must be aware that practical guides and other management tools for management are useful to guide our treatment of “patients like these” but are not enough to determine the treatment for “this patient”.
But attitude is not enough. In addition, we need to work at creating opportunities for conversation between clinicians and patients and that these become therapeutic relationships. I believe that our intellect has evolved in the taking of decisions with others. In the same way that I believe in deliberative democracy for social problems, I believe in taking shared decisions for clinical problems.
Clinical problems are not simple (such as in the problem of baking biscuits, with a known recipe and ingredients and an expected result), they are not complicated problems (like flying a 747, with algorithms and feedback that lets one be confident of achieving the desired result) but they are complex problems (like raising a child, with known ingredients, without a recipe or algorithms and with sometimes unexpected results).
Complex problems cannot be solved by technical investments only. These are solved within human relations. Specific results cannot be expected, but one can respond to adverse situations with resilience. Without the fuel of opportunity for this, the flame of a favourable attitude in the taking of shared decisions will be extinguished in the end.
The taking of shared decisions needs human relations between clinician and patient to resolve the human problems of the patient with resilience. In turn, the solution of these problems requires decisions to be shared for the solution to make intellectual, emotional and practical sense in the life of the patient.
Besides attitude and opportunity, it is important to have interpersonal skills (or train up to acquire whatever is possible) so as to communicate with a patient with empathy, to understand their situation and to assess each reasonable option in the context of a conversation.
In this context, tools based on evidence designed specifically to support these conversations can be useful and can facilitate the efficient taking of shared decisions in any context, from emergencies to specialised care.
I am aware that many have found the motivation to participate in taking shared decisions thanks to training or the use of tools for taking shared decisions. This makes it important to understand what is necessary and where so that taking shared decisions becomes routine practice in the care of patients.
But what does all this effort achieve? Many colleagues say that the taking of shared decisions can improve clinical outcomes, the adherence to treatments, the use of services and the costs of care. Taking shared decisions might also help in preventing global warming.
My critical appraisal of the evidence available does not allow me to discern any of these benefits with a sufficient level of certainty. This forces us to consider why we must thus make the effort to create the conditions to be able to take shared decisions and to implement this as routine practice.
For me, as a clinician, the answer comes by means of understanding the aim of a treatment, of clinical care as well as by allowing each patient to fulfil their dreams with the least pathological interruption and the least therapeutic inconvenience possible. To achieve this, we need to design treatments that respond to a patient’s situation – seen in high definition – treatments that make sense for the patient, and a clinician cannot do this without the patient.















 It is very common to see groups of people looking at their mobile devices in any place at any time: on holiday, at work, at home, in the underground, on the bus, in a congress, ….. wherever. It is also common to take advantage of our holidays to say that we will make the most of these days to disconnect from our routines. Does this include
It is very common to see groups of people looking at their mobile devices in any place at any time: on holiday, at work, at home, in the underground, on the bus, in a congress, ….. wherever. It is also common to take advantage of our holidays to say that we will make the most of these days to disconnect from our routines. Does this include 

