

The right to receive advice with regards to the information available on the network is reflected in the Carta de drets i deures de la ciutadania en relació a la salut i l’atenció sanitària (Citizens Bill of Rights and Duties relating to health and healthcare), updated in 2015. In particular, it specifies that a person has the right to obtain accurate and reliable recommendations from health professionals in terms of the available health information on the network (web pages, applications, etc…).
It is a fact that, from different professional sectors, we are more and more frequently identifying citizens as a key group to take into consideration when communicating the outcomes of our work, including the health sector. The different actors involved in disseminating health information resulting from the Catalan health system activity are no exception. When we publish our data we do it more and more in a way that is not only aimed at informing health professionals on the one hand but also at being accountable to citizens as end users.
But have we really asked citizens what information they want to obtain from us?
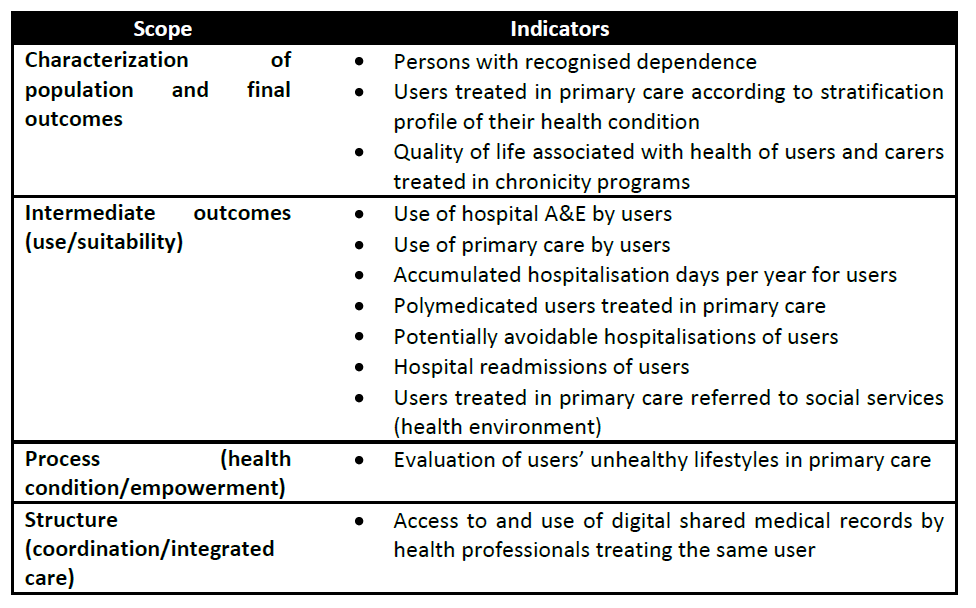
From the Results Centre of the Catalan Health System Observatory we publish a series of reports annually with quantitative indicators that aim to measure, assess and disseminate the results obtained in the different areas of the public health system. Up to the present, to disseminate this information beyond the comfort zone of the health sector, we have published a series of infographics with the information that we have considered to be most relevant for citizens, making the effort to create a user friendly format.

During the first semester of 2016, we spent time reflecting on our labour and we realised that we did not in fact know whether what we were publishing for citizens really reached or interested them. We did not even know what it was that citizens wanted to receive from us. To answer these questions we carried out a qualitative study of Catalan citizens to find out what their needs for health information were, but not limiting ourselves to that produced by the Results Centre.
We created three discussion groups and invited citizens randomly selected from Registre Central d’Assegurats del CatSalut (CatSalut’s Central Registry of the Insured) to freely express what they felt their necessities for health information were. What we discovered was that the population is not interested in receiving health information in a general or systematic way but rather only wants health information when they have a specific personal need and which is directly related to what is affecting them at a given time. They are not interested, therefore, in receiving health information about the population as a whole nor of how the health system works. They state that this information is necessary but feel it is health professionals who need to have it and know how to manage it. In this way, they place their trust in the health system by dissociating themselves from this type of information.
Furthermore, they consider it of interest that the information be made available on the networks but state that, whether they actively search for it on the internet or not, what they need is to be able to contrast the information at a later stage with their primary care physician or specialist, and that it be this professional who discerns what the best information available is for each occasion. What is more, they clearly identify this professional as being the person who needs to know the health information produced systematically by the Catalan health system.
We presented the results of this study at a recent congress, to be exact, the XXXIV Congress of the Spanish Society for the Quality of Healthcare and the XXI Congress of the Andalusian Society for the Quality of Healthcare, generating a very interesting posterior debate regarding these results. One of the attendees at the congress stated their concern for the fact that citizens were not interested in receiving general health information. The debate centred on how we could educate the population into showing an interest in this information and on how to make it reach them. We believe that the key underlying question here is whether this need be done at all.
The public at large have an overwhelming amount of information at their disposal on an infinite number of different subjects on a daily basis. It seems clear that when a person has a specific need regarding their state of health they consult a professional in whom they trust. It is obvious that to us, as healthcare professionals, we will always feel that the information we produce is of such interest as to make others want to know about it, but it is also probable that our enthusiasm makes us biased when interpreting reality. We should perhaps ask ourselves whether we need to make the effort to provide the public with information they say they do not need nor interests them, and whether we are prepared to accept their decision and respect it.
Post written by Dolores Ruiz-Muñoz, Anna García-Altés and Hortènsia Aguado.












")



 What has happened in periods of economic crisis has also occurred at other moments in time and in other contexts. It is also a well-known fact that this can lead to an increase in mortality rates among the population (both due to general causes, as well as for certain specific causes, such as suicide), an increase in mental health problems and a worsening of lifestyles. We also know that inequalities in healthcare can increase, particularly as the crisis affects the most vulnerable members of society first.
What has happened in periods of economic crisis has also occurred at other moments in time and in other contexts. It is also a well-known fact that this can lead to an increase in mortality rates among the population (both due to general causes, as well as for certain specific causes, such as suicide), an increase in mental health problems and a worsening of lifestyles. We also know that inequalities in healthcare can increase, particularly as the crisis affects the most vulnerable members of society first.