In a previous post we discussed the advantages of using indicators in the assessment of health services. At AQuAS we have been applying indicators to assess different care processes and areas, with care for patients suffering from chronic conditions being one of the principal areas of interest in terms of new care models and programs assessment. Interventions in the field of care for chronicity are extremely complex given that by their very nature, they tend to involve multiple actors and many different levels of care concurrently, as well as different elements utilising therapeutic instruments and technology with very variable intensity. Moreover, their effectiveness is often linked to contextual factors, making it difficult to attribute an outcome to a particular component of the program. So, given this level of complexity, the question remains, why should we be using indicators in this area? The answer is that these indicators may provide us with several benefits compared to other assessment approaches, such as:
- Incorporating professional opinion and consensus
- The possibility of including structural and procedural indicators allows us to obtain an understanding of the environment and the reality in which the initiative is being implemented
- Providing a type of assessment that is more accessible and understandable for professionals
- Greater simplicity and speed in evaluation and obtaining results
- Possibility of defining standards
- Allowing comparisons to be established and objectifying trends
- Identifying successful characteristics and factors that can define which models are most effective, for which groups of chronic patients, in what context and at what cost
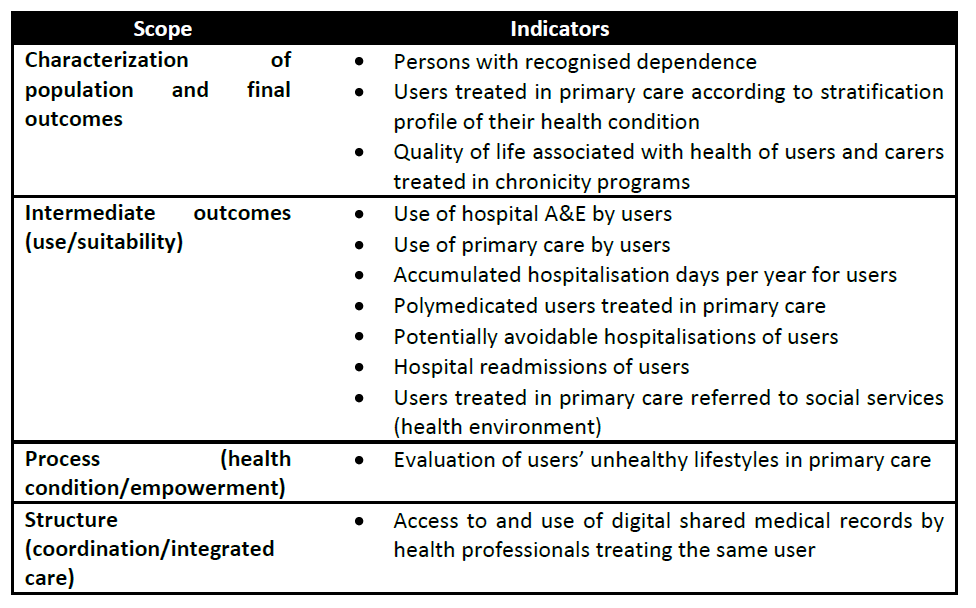
The first project in which AQuAS began using quality of care indicators for assessing chronicity got underway in 2012 with the commission by the Program for Prevention and Care for Chronicity (PPAC) to define a set of indicators to assess the quality of integrated care programs for chronicity within the health sector, where an ‘integrated program’ is understood as those programs involving the coordinated participation of different levels of care. Following the methodology described in the previous post (review of literature, establishing a theoretical framework and expert opinions) a total of 18 indicators were obtained, mainly from intermediate and final results, which experts considered relevant and feasible for assess these types of programs and which are currently being implemented (see table 1 and web).
Table 1: Indicators assessed as relevant and feasible for evaluating integrated care programs for chronicity

From this experience, AQuAS developed a proposal for indicators, published recently to, assess chronic care as part of the strategy for tackling chronicity within the National Health System. As a result of this work, a set of indicators considered to be crucial for evaluation emerged, which included several previously prioritized indicators which are repeated such as polymedication, avoidable readmissions and hospitalisations, but which incorporates new factors which are more closely associated with the patients’ experience, such as the assessment of the patients’ and carers’ quality of life, or patients’ lifestyles (see Table 2).
Table 2: Proposal for prioritized indicators for promoting more uniform measurement of the entire National Health System for evaluating of chronicity care strategies
Later, from 2014 onwards, the Catalan Institute of Healthcare and Social Services (ICASS – Dpt. Social Welfare and Family) and the PPAC (Health Dept.), commissioned extensive work to be carried out in evaluating collaborative social and health care models in Catalonia. These models not only consider the different levels of care in the health system but also include social services, a crucial aspect in caring for patients in this category. The objectives of the project were to outline the organization and operations of these collaborative experiences, identify barriers and facilitators, propose a conceptual framework for assessment and define a set of well-founded indicators based on feedback from participants and the expertise acquired from previous assessment studies. The proposed indicators continue to take into account traditional indicators while consolidating assessment that includes the views of those involved, not just the patient, but also the caregivers and professionals, and placing special emphasis on the evaluation of the coordinated actions of healthcare and social services, for example considering the avoidance of duplicate processes or carrying out joint social and healthcare initiatives.
We must also highlight in this line of work the efforts undertaken by the ITES FORUM (Forum of innovation, transformation and excellence in health and social services) to define a joint health and social services evaluation framework with a proposal of indicators (line L6) and in which AQuAS is also involved jointly with professionals from different fields. The Forum is a tool to facilitate the necessary conceptual debate required for transforming existing social services and healthcare in favour of a new model of integrated care.
Finally, and to continue discussing the area of assessing the integration of health and social services, since 2015 AQuAS has been involved in the Horizon2020 SUSTAIN (Sustainable tailored integrated care for older people in Europe) project. This European project aims to compare, assess and implement strategies to improve integrated care experiences aimed at non-institutionalized elderly individuals, in other words, those living in their own homes. The project has an additional goal, which is to seek to ensure that the best integrated care initiatives in this area are applicable and adaptable to other European health systems and regions. The project involves seven European countries working simultaneously on the basis of the definition and implementation of a set of indicators pending definition, tailored to this type of population and integrative approach.
Indicators, therefore, are useful tools for assessing an area as large and as complex as chronicity and they can be applied from a broader or narrower perspective, in other words, taking into account not only the different levels of care in the health system, but also including social services. The results obtained from the implementation of these indicators will provide professionals with objective criteria regarding the quality of their interventions, by facilitating the identification of the strengths of chronic care programs, as well as areas with scope for improvement.
Post written by Noemí Robles, Laia Domingo i Mireia Espallargues. Àrea d’Avaluació, AQuAS.